The main findings from this report include the following:
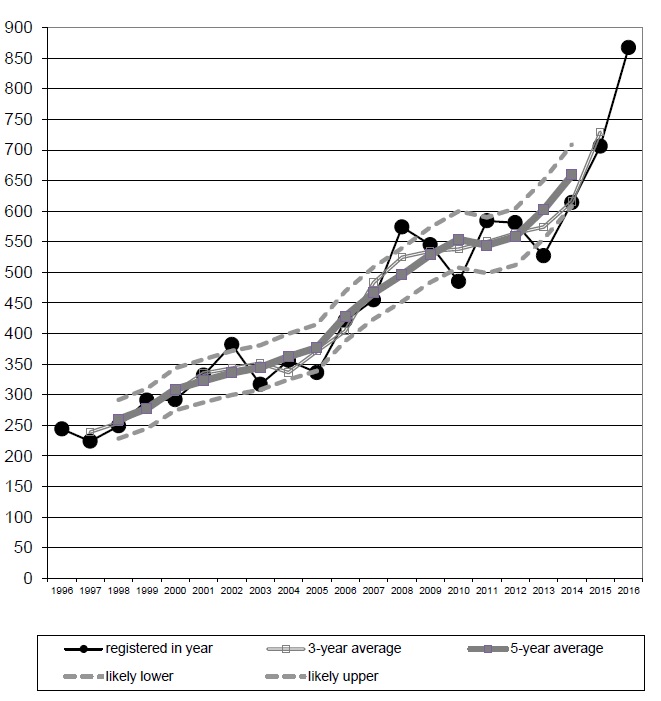
Based on the definition used for these statistics, 867 drug-related deaths were
registered in Scotland in 2016, 161 (23%) more than in 2015. This was the largest
number ever recorded, and 446 (106%) higher than the figure for 2006, which was
421 (paragraph 3.1.1).
Males accounted for 68% of the drug-related deaths in 2016 (paragraph 3.4.1).
In 2016, there were 327 drug-related deaths of people aged 35-44 (38% of all
drug-related deaths), 213 in the 45-54 age-group (25%), and 199 drug-related
deaths of 25-34 year olds (23%). There were 42 drug-related deaths at ages 15-24
(5%), and 66 of 55-64 year olds (8%) (paragraph 3.4.2).
The NHS Board areas which accounted for most of the 867 drug-related deaths in
2016 were:
Using the annual average for 2012-2016, to reduce the effect on the figures of year-to-year fluctuations:
for Scotland as a whole, the average of 659 drug-related deaths per year
represented a death rate of 0.12 per 1,000 population;
the NHS Board area with the highest rate was Greater Glasgow & Clyde (0.17);
the next highest rate was for Ayrshire & Arran and Tayside (both 0.13) paragraph 4.3.
However, there is a narrower (in percentage terms) range of values when death rates are
calculated using the estimated numbers of problem drug users (paragraph 4.9).
Comparing the annual average for 2012-2016 with that for 2002-2006:
the percentage increase in the number of drug-related deaths was greater for
females (169%) than for males (60%) (paragraph 3.4.1);
the largest increase in numbers was for 35-44 year olds, the next largest was for
people aged 45-54, and there was a fall in the number of drug-related deaths of
people aged under 25 (paragraph 3.4.2); and
the NHS Board areas with the largest increases in the number of drug-related
deaths were Greater Glasgow & Clyde (up by 61), Lothian (up by 59) and
Lanarkshire (up by 40) (paragraph 4.2).
The standard basis for the figures for individual drugs for 2008 and subsequent years is
‘drugs which were implicated in, or which potentially contributed to, the cause of death’. Of
the 867 drug-related deaths in 2016:
heroin and/or morphine were implicated in, or potentially contributed to, the cause of
473 deaths (55% of the total);
methadone was implicated in, or potentially contributed to, 362 deaths (42%);
one or more opiates or opioids (including heroin/morphine and methadone) were
implicated in, or potentially contributed to, 765 deaths (88%);
benzodiazepines (for example diazepam, diclazepam and etizolam) were implicated
in, or potentially contributed to, 426 deaths (49%);
cocaine, ecstasy-type drugs and amphetamines were implicated in, or potentially
contributed to, 123 deaths (14%), 28 deaths (3%) and 25 (3%) deaths, respectively;
and
alcohol was implicated in, or potentially contributed to, 112 of the drug-related
deaths (13%) (paragraph 3.3.3).
(The percentages add up to more than 100 because more than one drug was implicated
in, or contributed to, many of the deaths.)
In 2016, heroin and/or morphine were implicated in, or potentially contributed to, more
deaths than in any previous year (hitherto, the largest figure had been 345 in 2015). The
number for methadone was also above its previous peak (275 in 2011), as was the case
for opiates or opioids (including heroin/morphine and methadone) as a group (previous
highest figure 606 in 2015) and for benzodiazepines as a group (previous highest levels
of 196 in 2012, and - on the basis used before 2008 - 245 in 2002) (paragraph 3.3.4).
Most drug-related deaths are of people who took more than one substance. Of the 867
drug-related deaths in 2016, there were just 66 for which only one drug (and, perhaps,
alcohol) was found to be present in the body. There were 187 cases where only one drug
(and, perhaps, alcohol) was believed to have been implicated in, or potentially contributed
to, the cause of the death. The latter figure covers both the ‘only one drug found’ deaths
and cases where one drug was implicated and the other drugs present were not
considered to have had any direct contribution to the death (paragraph 3.3.9 to 3.3.11)
Annex E of this publication provides information about deaths which involved so-called
‘New Psychoactive Substances’ (NPSs). The definition used for the purpose of those
figures is set out in first half of that Annex. On that basis, in 2016:
there were 286 deaths for which NPSs were implicated in, or potentially contributed
to the cause of death. In 277 cases, the only NPSs present were benzodiazepines
(usually etizolam, but sometimes – for example - diclazepam or phenazepam); in
eight cases, other types of NPS were present (for example PMA, PMMA and MXP);
there was one death for which both benzodiazepine NPSs and other types of NPS
were present. Almost all of these deaths (281 out of 286) fall within the definition of
‘drug-related deaths’ that is used to produce the main statistics in this report – this
means they are included in the 867 drug-related deaths. In only a small proportion (4
out of the 286 deaths) were NPSs the only substances implicated in the death.
(paragraph E9)
there were 60 deaths for which NPSs were present but were not considered to have
contributed to the death. In all cases, the only NPSs present were benzodiazepines;
almost all of the deaths (59 out of 60) are included in the 867 drug-related deaths (paragraph E11).
Figure 1: Drug-related deaths in Scotland, 3- and 5-year moving averages, and
likely range of values around 5-year moving average